
1
New Mexico Child Fatality Review 2023
Report
Findings & Recommendations from Child Deaths Reviewed in 2022
Oice of Injury and Violence Prevention
Injury and Behavioral Epidemiology Bureau
Epidemiology and Response Division
New Mexico Department of Health
December 2023
2
This page intentionally left blank.

3
State of New Mexico
The Honorable Governor Michelle Lujan Grisham
New Mexico Department of Health
Patrick Allen, Cabinet Secretary
Laura Chanchien Parajón, MD, MPH, Deputy Cabinet Secretary
Epidemiology and Response Division
Laura Chanchien Parajón, MD, MPH, Acting Division Director
Heidi Krapfl, MS, Deputy Division Director of Programs
Injury and Behavioral Epidemiology Bureau
Rachel Wexler, Acting Bureau Chief
Oice of Injury and Violence Prevention
Rachel Wexler, Injury & Violence Prevention Section Manager
Rachel E. Ralya, Evaluation Unit Manager
Oluwatosin Ogunmayowa, PhD, Senior Injury Epidemiologist
Arpita Paul, MPH, MBBS, Injury Epidemiologist
4
Table of Contents
Executive Summary........................................................................................................................................ 5
Background .................................................................................................................................................... 7
Child Fatality Review .................................................................................................................................. 7
A Framework for Prevention ....................................................................................................................... 8
A Public Health Approach ....................................................................................................................... 8
Social-Ecological Model.......................................................................................................................... 9
Shared Risk and Protective Factors ........................................................................................................ 9
Social Determinants of Health ...............................................................................................................10
Adverse Childhood Experiences ............................................................................................................ 11
New Mexico Child Fatality Review ............................................................................................................. 13
Review Panels ........................................................................................................................................14
Report Narrative ............................................................................................................................................ 15
Child Death in New Mexico ........................................................................................................................ 15
Leading Causes of Child Death.............................................................................................................. 15
The Cost of Child Mortality .................................................................................................................... 17
Child Injury Death Rate .......................................................................................................................... 18
Youth Mental Health in New Mexico ..........................................................................................................19
Disparities in Youth Suicide Aempts................................................................................................... 20
Child Fatalities Reviewed by NM-CFR ........................................................................................................ 21
2023 Report ............................................................................................................................................. 24
Methodology ........................................................................................................................................ 24
Materials Reviewed............................................................................................................................... 24
Panel Reviews ....................................................................................................................................... 25
Shared Risk and Protective Factors for Child Fatality in NM .................................................................. 45
Limitations ............................................................................................................................................ 48
Conclusions .......................................................................................................................................... 48
NM-CFR Recommendations ..................................................................................................................... 49
Previous Recommendations ................................................................................................................. 49
Discussion of Recommendations ......................................................................................................... 50
Key Recommendations .......................................................................................................................... 51
Appendix .................................................................................................................................................. 52
Appendix A: Acknowledgements .......................................................................................................... 52
Appendix B: State of New Mexico Child Death Review Legislation ....................................................... 55
Appendix C: Glossary Terms from OMI 2021 Annual Report.................................................................... 56
Appendix D: Oice of the Medical Investigator Annual Report 2021 – Excerpt (page 44)..................... 57
Appendix E: Suicide Awareness, Prevention and Training Organizations ............................................. 58
Appendix F: New Mexico Rule for Small Numbers and Public Data Release .......................................... 59
Appendix G: Related Resources ........................................................................................................... 60
References............................................................................................................................................... 62
NM-CFR 2023 Report Tear Sheet ............................................................................................................. 64

5
Executive Summary
The New Mexico Child Fatality Review (NM-CFR) was established in 1998, with the implementation of
Title 7 of the New Mexico Administrative Code (NMAC) Chapter 4- Disease Control, Part 5, Maternal,
Fetal, Infant and Child Death Review (NMAC 7.4.5) to examine the factors that contribute to the death
of children in New Mexico (NM) (see Appendix B). All non-natural child resident deaths in NM are
subject to review by NM-CFR. Deaths due to intentional (suicides, homicides) and unintentional
injuries (drowning, suocation, motor vehicle crashes) are preventable and vary by age. These deaths
undergo a thorough review process by multidisciplinary review panels, allowing stakeholders to beer
understand the circumstances surrounding these deaths. Through the review process, panelists
identify gaps in systems, as well as risk and protective factors of child fatalities, and develop
actionable recommendations to prevent future child fatalities of similar circumstance.
The NM-CFR utilizes the National Center for Fatality Review and Prevention (NCFRP) steps to conduct
eective review meetings:
The NM-CFR 2023 Report summarizes and analyzes information about 84 unique injury-related
deaths of NM infants, toddlers, children, and youth under the age of 18, which were reviewed in 2022.
The child fatalities described in this report occurred between the years 2018 and 2022 and includes: 2
child deaths that occurred in 2018, 7 deaths that occurred in 2019, 29 deaths that occurred in 2021, 43
deaths that occurred in 2021, and 3 deaths that occurred in 2022.
This report should not be used to compare changes over time to previous CFR reports published
by the NMDOH Oice of Injury and Violence Prevention.
Such a comparison would be inaccurate
because of the overlap in year of death.
6
Report Highlights
Causes of Death
Of the 84 unique child fatalities reviewed in 2022 and analyzed in this report, the leading causes of
death were: asphyxiation (30%), bodily force or weapon (27%), unknown (20%), and motor vehicle
crashes (11%), followed by poisoning (5%), drowning (3%), and other incidents (3%).
Age, Gender and Race
Of the 84 unique child fatalities reviewed in 2022 and analyzed in this report, the age group with the
most deaths was infants under the age of one (n=35), child fatalities were markedly higher in males
(n=54) and nearly half of cases reviewed (n=41) were of Hispanic or Latino ethnicity.
Location of Death
Of the 84 unique child fatalities reviewed in 2022 and analyzed in this report, the highest number of
child deaths were found in Bernalillo County, with 23 cases (27.8%). Following that, seven cases
(8.3%) were out of Doña Ana County, and six cases (7.14%) were out of San Juan County.
Preventability
Of the 84 unique child fatalities reviewed in 2022 and analyzed in this report, NM-CFR determined
that 80% (n=67) could have been prevented, and 2% of deaths (n=2) couldn’t be prevented.
Key findings from cases reviewed can be found in the 2023 Report, beginning on page 24.
Recommendation Highlights
In response to the data provided in this report, the NM-CFR makes evidence-based recommendations
to prevent future child fatalities of similar circumstances:
• to support program operations and improve the data used for the review,
• to increase awareness of the burden of child fatality and prevention eorts,
• to increase safe home environments, and
• to increase behavioral healthcare and access to resources.
A more detailed list of prevention recommendations can be found in the NM-CFR Recommendations
section, beginning on page 49.
The NM-CFR 2023 Report Tear Sheet is a one-page summary resource at the end of this report,
beginning on page 65. For optimal use, print in color and on both sides.

7
Background
Child Fatality Review
Every year, over 37,000 children in the United States die before reaching the age of 18. The death of a
child is a great loss to family and community. One indicator of a society's general well-being is the
ability to lower child death rates.
Child fatality review is a process in which multidisciplinary teams meet to share and discuss
information collected about a child death, also referred to as case information, to understand the
circumstances around child deaths. These multidisciplinary commiees are made up of
representatives from the medical community, public health, law enforcement, child protective
services, the oice of the coroner/medical examiner, and the prosecuting aorney's oice.
Local, regional, and state teams throughout the United States and its territories then submit this
information to the National Fatality Review Case Reporting System, a database managed by the
National Center for Fatality Review and Prevention
(NCFRP).
The Child Fatality Review process aims to:
• Identify risk and preventable causes of illness or injury
• Develop actionable recommendations to prevent child death
• Disseminate findings and recommendations to partners in prevention
The information included in this report is accessed from the New Mexico Department of Health
(NMDOH) BVRHS and from the NCFRP National Fatality Review Case Reporting System database,
which is funded by the US Department of Health and Human Services. The state, regional, and local
governments, healthcare providers, child-serving and educational groups, communities, and families
can use this information to guide decisions to make their communities safer and prevent further child
fatalities.

8
A Framework for Prevention
A Public Health Approach
Public health is “the science and art of preventing disease, prolonging life, and promoting health
through the organized eorts and informed choices of society, organizations, public and private
communities, and individuals.” — CEA Winslow
Public health is focused on improving health outcomes for entire populations. It is a science which
draws on an evidence-base informed by numerous disciplines, including medicine, epidemiology,
social sciences, education, and economics. The New Mexico Department of Health uses a public
health approach to 1) Define and Monitor the Problem, 2) Identify Risk and Protective Factors 3)
Develop and Test Prevention Strategies and 4) Assure Widespread Adoption.
Similarly, this public health approach to prevent child fatalities seeks to improve the health and
wellbeing of all children under 18 years of age. As part of this approach, NM-CFR conducts a review
process to identify factors which increase or decrease the risk of injury or violent victimization, also
called risk and protective factors. Based on this review, prevention strategies are developed through
the recommendation process.
Figure 1. The Public Health Approach

9
Social-Ecological Model
The Social-Ecological Model (SEM) considers the dynamic interplay of factors which influence health
at and across multiple levels of society- individual, relationship, community, and societal.
To improve health outcomes and to remove the burden of child fatalities, risk and protective factors
are identified at each level of the SEM. Findings and recommendations are developed for each case,
considering unique characteristics at each level of the SEM.
Shared Risk and Protective Factors
Shared Risk and Protective Factors (SRPF) is a term used in public health to acknowledge factors
which either increase or decrease interconnected risks of injury. These risk and protective factors
may occur at any singular or on multiple levels of the Social-Ecological Model.
Figure 2. The Social-Ecological Model

10
Social Determinants of Health
Social determinants of health (SDOH) are the non-medical factors that have impacts on health
outcomes and contribute to a wide range of health disparities (CDC, 2023). SDOH play a crucial role in
influencing the overall health and well-being of individuals, regardless of their age.
However, it is especially crucial to consider the influence of SDOH on children and youth. This is
because the physical, social, and emotional abilities that develop during early life serve as the
building blocks for long-term health and well-being throughout the lifespan. Health disparities exist in
the population of NM among dierent racial, ethnic, and socioeconomic groups due to inequitable
dierences in SDOH.
Source: Healthy people 2030, US department of Health and Human Services
The NM-CFR considers various interconnected factors operating at dierent levels during case
reviews. These factors encompass educational aainment, economic stability, social and community
dynamics, neighborhood characteristics, access to healthcare, and policy influences.
Figure 3. Social Determinants of Health
11
Adverse Childhood Experiences
Adverse childhood experiences (ACEs) refer to potentially traumatic events that take place during
childhood (ages 0-17 years). Neighborhoods lacking resources or experiencing racial segregation
have the potential to induce stress which compounds the eect of ACEs on the development of
children's brains, immune systems, and stress-response systems. ACEs also disrupt a child’s ability to
develop healthy aention spans, decision-making processes, and ability to learn, while increasing the
risk of injury-related deaths (CDC, 2023), and the risk of future violence victimization and/or
perpetration.
The Centers for Disease Control and Prevention (CDC) categorizes ten ACEs into three groups:
abuse, neglect, and household challenges (CDC, 2021). The ten ACEs are:
• Abuse
o Emotional abuse: A parent, stepparent, or adult living in your home swore at you,
insulted you, put you down, or acted in a way that made you afraid that you might be
physically hurt.
o Physical abuse: A parent, stepparent, or adult living in your home pushed, grabbed,
slapped, threw something at you, or hit you so hard that you had marks or were injured.
o Sexual abuse: An adult, relative, family friend, or stranger who was at least 5 years
older than you ever touched or fondled your body in a sexual way, made you touch
his/her body in a sexual way, aempted to have any type of sexual intercourse with
you.
• Household Challenges
o Mother treated violently: Your mother or stepmother was pushed, grabbed, slapped,
had something thrown at her, kicked, bien, hit with a fist, hit with something hard,
repeatedly hit for over at least a few minutes, or ever threatened or hurt by a knife or
gun by your father (or stepfather) or mother’s boyfriend.
o Substance abuse in the household: A household member with excessive use of
psychoactive drugs, such as alcohol, pain medications, or illegal drugs that can lead to
physical, social or emotional harm.
o Mental illness in the household: A household member was depressed or mentally ill or
a household member aempted suicide.
o Parental separation or divorce: Your parents were ever separated or divorced.
o Incarcerated household member: A household member went to prison.
•
Neglect
o
Emotional neglect: Someone in your family never or rarely helped you feel important or
special, you never or rarely felt loved, people in your family never or rarely looked out for
each other and felt close to each other, or your family was never or rarely a source of
strength and support.
o
Physical neglect: There was never or rarely someone to take care of you, protect you,
or take you to the doctor if you needed it, you didn’t have enough to eat, your parents
were too drunk or too high to take care of you, or you had to wear dirty clothes.

12
Emerging research about additional circumstances experienced in childhood which may increase
adversity:
• Housing insecurity
o Emerging research suggests that adults who have experienced housing insecurity are
significantly more likely to have encountered adverse experiences during their
childhood compared to individuals in the general population who have not experienced
housing insecurity (Curry, 2017).
• Community violence
o Experiencing community violence and physical abuse during childhood can have a
significant impact on both externalizing behaviors and academic performance in later
years. Furthermore, it is crucial to acknowledge that community violence exposure
(CVE) has a distinct and autonomous eect when evaluating the influence of physical
abuse (Schneider, 2020).
ACEs and the detrimental eects they cause can be reduced through preventive measures. The
establishment and maintenance of secure, stable, and nurturing relationships and environments for
children and families can eectively mitigate ACEs and reduce the occurrence of child fatalities. In
2019, the Centers for Disease Control and Prevention issued a resource guide about ACEs
,
highlighting six strategies to prevent ACEs:
1. S
trengthen Economic Supports for Families;
2. Promote Social Norms that Protect Against Violence and Adversity;
3. Ensure a Strong Start for Children;
4. Teach Skills;
5. Connect Youth to Caring Adults and Activities;
6. Intervene to Lessen Immediate and Long-term Harms.
Essentials for Childhood: Preventing Adverse Childhood Experiences through Data to Action i
s a CDC
funded program focused on preventing ACEs and promoting positive childhood experiences (PCEs).
Twelve recipient organizations across the nation are building or improving ACEs and PCEs data
collection infrastructure and capacity, implementing and sustaining ACEs prevention strategies,
focusing on health equity and conducting ongoing data-to-action activities to inform changes to
their existing prevention strategies or select additional strategies.
13
New Mexico Child Fatality Review
Title 7 of the New Mexico Administrative Code (NMAC) Chapter 4- Disease Control, Part 5, Maternal,
Fetal, Infant and Child Death Review (NMAC 7.4.5) to examine the factors that contribute to the death
of children in NM (see Appendix B).
The NM-CFR employs a confidential, comprehensive approach, incorporating both qualitative and
quantitative data related to non-natural child deaths, which includes accidental deaths, homicides by
parent or caregiver, suicides, and cases where the cause of death cannot be determined. Homicides
by a person other than a parent or caregiver are excluded from review. All non-natural child deaths in
NM are subject to review by NM-CFR. The objective of this approach is to improve understanding of
the complex variables associated with child fatalities in the state of New Mexico.
These deaths undergo a thorough review process by multidisciplinary review panels, allowing
stakeholders to beer understand the circumstances surrounding these deaths. Through the review
process, panelists identify gaps in systems, as well as risk and protective factors of child fatalities,
and develop actionable recommendations to prevent future child fatalities of similar circumstance.
The review process can also alert communities and policy makers about emerging trends in
circumstances surrounding intentional and unintentional injuries which contribute to child deaths.
For more than 20 years, NM-CFR has been providing prevention recommendations. While some of the
recommendations led to enacted legislation, many of the recommendations were adopted by state
agencies and community partners. NM-CFR reports from previous years may be found at
www.nmhealth.org
.
Standard definitions of fatality-related terms, including manner of death (Appendix C), provided in
the New Mexico Oice of the Medical Investigator 2021 Annual Report
, describe data points that are
referred to in the death certification processes and used by NM-CFR (Appendix D). The New Mexico
Rule for Small Numbers and Public Data Release (Appendix F) guides the suppression of specific data
in this report as necessary.

14
Review Panels
In 2022, NM-CFR maintained four distinct case review panels. Each panel is comprised of a diverse
group of experts in child safety, public health, education, behavioral health, medicine, forensic
pathology, law enforcement, public safety, juvenile and criminal justice, and other related fields.
Child Abuse, Neglect
or Homicide (CAN-H)
This panel reviews child fatalities that result from
parent/caregiver abuse, neglect or homicide.
Sudden Unexpected
Infant Death (SUID)
This panel reviews unexpected deaths of infants less than one
year old in which the cause was not obvious before investigation.
Unintentional Injury
This panel reviews child fatalities in which the manner of death
was accidental or undetermined. The causes of death are varied
and include motor vehicle crashes, drownings, unintentional
overdose or poisonings, fire or environmentally related, and other
unintentional injuries.
Youth Suicide
This panel reviews intentional deaths among children and youth
that result from self-injury.

15
Report Narrative
This report analyzes characteristics of child fatalities reviewed in calendar year 2022. A supplemental
analysis of cases reviewed by death year(s) is presented in Figures 7, 8 and 9.
This report aims to provide information about child fatality in NM, and to promote the widespread
adoption of prevention strategies and recommendations by the NM-CFR. Its primary goal is to
advocate for the widespread implementation of prevention strategies and recommendations
endorsed by the NM-CFR. The collaborative expertise of multidisciplinary panels enhances the
likelihood of formulating pertinent and influential recommendations, ultimately influencing health
outcomes within this demographic.
Child Death in New Mexico
Leading Causes of Child Death
The following tables present the primary cause of child mortality in New Mexico from 2011 to 2021.
These data represent all child fatalities in NM, including both those due to natural causes and non-
natural causes. The table shows that unintentional injury (also referred to as accidents) consistently
ranked as the foremost cause of death during this period. Suicide and homicide have been identified
as the fourth and fifth leading causes of death in children 0-17 years of age over the course of these
years. Upon analysis across various age groups, it was discovered that injury-related deaths
consistently ranked among the leading five causes of death for children.
Table 1. Leading Causes of Child Deaths in New Mexico, 2011-2021
Leading Cause-
Children 0-17 Years
of Age
Number of Deaths
Crude rate per
100,000
population
Percentage of all
Child Deaths in
NM
Unintentional Injury
589
10.82
35.5%
Congenital Anomalies
432
7.94
26.0%
Short Gestation
276
5.07
16.6%
Suicide
231
4.24
13.9%
Homicide
133
2.81
8.0%
Source: WISQARS™ — Web-based Injury Statistics Query and Reporting System (Last accessed: December 7,
2023)
Analysis of the causes of all childhood deaths in NM from year 2011 to 2021 found that unintentional
injuries were the top cause of death across multiple age groups (1 to 4 years, 5 to 9 years, 10 to 14
years, and 15 to 17 years) and the third leading cause of death in infancy (less than one year of age).
Suicide was found to be the second leading cause of death in 10 to 14 years and 15 to 17 years age
group. Homicide was the third leading cause of death in 1 to 4 years, 5 to 9 years, and 15 to 17 years
age groups. In the 5 to 9 years age group, Homicide and congenital anomalies both ranked in the

16
same position. Homicide was also found to be the fourth leading cause of death in the 10 to 14 years
age group (Table 2).
Table 2. Leading Causes of Death and Percentage by Age Group in New Mexico, 2011-2021
Leading
cause of
Death
<1 year
1 to 4 years
5 to 9 years
10 to 14 years
15 to 17 years
1
Congenital
Anomalies
39.7%
Unintentional
Injury
59.0%
Unintentional
Injury
50.6%
Unintentional
Injury
36.5%
Unintentional
Injury
40.4%
2
Short
Gestation
31.4%
Congenital
Anomalies
14.5%
Malignant
Neoplasms
18.2%
Suicide
33.3%
Suicide
37.3%
3
Unintentional
Injury
12.5%
Homicide
13.3%
Homicide
*
Malignant
Neoplasms
13.1%
Homicide
13.9%
4
Maternal
Pregnancy
Complication
s
9.3%
Malignant
Neoplasms
*
Congenital
Anomalies
*
Homicide
9.5%
Malignant
Neoplasms
*
5
Placenta Cord
Membranes
7.1%
Influenza &
Pneumonia
*
Chronic Low.
Respiratory
Disease &
Septicemia
*
Congenital
Anomalies
*
Congenital
Anomalies
*
U Unintentional Injury ry Suicide Homicide
Non-injury Deaths
Source: WISQARS™ — Web-based Injury Statistics Query and Reporting System Last accessed: December 7,
2023
* Indicates suppressed values (Small Numbers Rule, Appendix F)

17
The Cost of Child Mortality
Injury-related fatalities not only carry an immeasurable impact on individuals, families, and society,
but they also generate economic impacts. The expenses associated with injury-related fatalities
encompass medical expenditures linked to deaths caused by injuries and the value of statistical life,
which is a monetary assessment of the overall value individuals place on reducing the risk of mortality.
Value of statistical life represents the ratio of financial considerations to the risk of death. It functions
as an indicator that assesses the marginal cost of improving safety and the population's readiness to
pay for preventive and risk reductive measures. The values displayed in Table 3 are estimates based
on the age of the child at time of death. For individuals aged 0-17 years, the assigned value was 16.9
million U.S. dollars, which was derived by adjusting the estimate based on life expectancy and
baseline quality of life among population (CDC, 2021).
Table 3. Fatal Injuries in Children and Associated Cost in New Mexico, 2021
Year
Number of
Injury related
deaths (0 to
17 years)
Total
Medical
Costs
Total Value of
Statistical Life
Total
Combine
d cost
2018
97
$906,009
$1.78 B
$1.78 B
2019
102
$865,081
$1.87 B
$1.87 B
2020
85
$837,323
$1.56 B
$1.56 B
2021
110
$1.34 M
$2.01 B
$2.01 B
Source: WISQARS™ — Web-based Injury Statistics Query and Reporting System Last accessed: December 7,
2023
While value of statistical life estimates the economic burden of premature death, there is no manner
to quantify the social, psychological, and emotional impacts of the loss of a child’s life on their family,
friends and community. NM-CFR acknowledges that a statistical life estimate does not represent the
complete value of the lives lived.

18
Child Injury Death Rate
The child injury death rate in NM has consistently been higher than the national rate. Figure 4 shows
that the child injury-related death rate in NM was 16.2 per 100,000 population in 2011, while the US
rate was 11.8 per 100,000 population. In 2021, the injury related death rate was 23 per 100,000
population in NM compared to 14.4 per 100,000 population in the US.
Source: CDC WONDER, Last accessed: October 17, 2023
The percentage difference in rates between NM and the US for child injury related deaths was 37.8%
in 2011, and it increased to 59.7% in 2021. From 2011 to 2021, a 41% increase was observed for child
injury-related deaths in NM.
11.8
14.4
16.2
23
0
5
10
15
20
25
2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021
Crude rate per 100,000 population
Year
US New Mexico
+41% NM
(2011-2021)
2011
NM vs. U.S.
crude rate:
+37.8%
2021
NM vs. U.S.
crude rate:
+59.7%
Figure 4. Crude Rate (per 100,000 population) for All Injury-related Fatalities for Children (ages 0-17) in
New Mexico and the United States, 2011-2021
19
Youth Mental Health in New Mexico
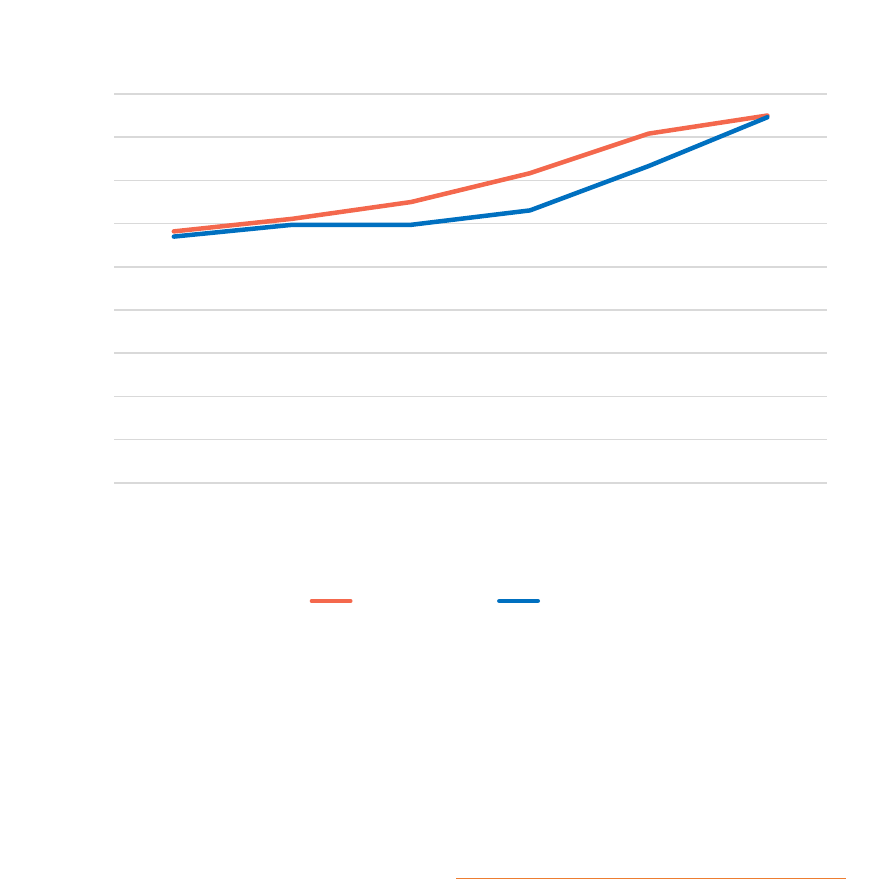
According to data captured by the NM Youth Risk & Resiliency Survey (YRRS), in 2021, two out of five
NM high school students and three out of five NM female high school students experienced
persistent feelings of sadness or hopelessness, an overall increase of 44% since 2011 (YRRS). Figure 5
illustrates an increase in feelings of persistent sadness or hopelessness in New Mexican high
schoolers compared to the national average from 2011 to 2021.
Source: 2011-2021 NMYRRS (NMDOH); and 2011-2021 National YRBS (CDC)
Suicide is the second leading cause of death for 10 to 14-year-olds and the third leading cause of
death among individuals between the ages of 15 to 24 years in the United States (CDC, 2023).
In 2021, the Surgeon General, Vivek Murphy, issued a health advisory on youth mental health, writing,
“ensuring healthy children and families will take an all-of-society eort, including policy, institutional,
and individual changes in how we view and prioritize mental health.
29%
42%
28%
42%
0
5
10
15
20
25
30
35
40
45
2011 2013 2015 2017 2019 2021
% Percent
Persistently Felt Sad or Hopeless
New Mexico US
Figure 5. Persistently Felt Sad or Hopeless, Grades 9-12, New Mexico, and United States

20
Disparities in Youth Suicide Aempts
Risk for suicide aempts was highest among transgender, genderqueer, genderfluid students as well
as students identifying as lesbian, gay, bisexual, or questioning. American Indian or Alaska Native high
school students were 56% more likely to have aempted suicide than White peers (Figure 6).
Error Bar indicates 95% confidence interval.
Source: 2021 NMYRRS
14%
7%
14%
12%
13%
10%
8.7%
9%
31%
8%
21%
10%
0 5 10 15 20 25 30 35
Female
Male
American Indian or Alaska Native
Asian or Pacific Islander
Black or African American
Hispanic
White
Other Gender
Transgender, Genderqueer, or Genderfluid
Other Sexual Orientation
Lesbian, Gay, Bisexual, or Questioning
Total
Sex Race/Ethnicity
Gender
Identity
Sexual
Orientation Total
% of Suicide attempts
Figure 6. Percent of High School Students Who Aempted Suicide, by Demographics, 2021

21
Child Fatalities Reviewed by NM-CFR
Figure 7 indicates the distribution of manner of death in the reviewed cases of injury-related deaths
among children aged 0-17 years in NM, from 2005 to 2022. Most deaths which were reviewed by NM-
CFR were due to unintentional injury, followed by suicide, undetermined deaths, homicide, natural,
and deaths with unknown
1
causes.
Source: N CF RP, Last accessed: October 3, 2023
1
For the purpose of this analysis, “undetermined” cases are a classification by the Oice of the Medical Investigator, where
the cause of death was not able to be determined, whereas unknown cases are those in which there was limited information
or a null value.
Figure 7. Child Fatalities Reviewed by NM-CFR, by Manner of Death in New Mexico, 2005- 2022
Unknown, 3%

22
By count, the highest number of cases reviewed by NM-CFR in 2022 were from Bernalillo County
(n=318), followed by San Juan County (n=100), McKinley County (n=80), Doña Ana County (n=76),
and Sandoval County (n=71) (Figure 8).
Source: N CF RP, Last accessed: October 3, 2023
Figure 8. Child Fatalities Reviewed by NM-CFR, by County in New Mexico, 2005-2022

23
The distribution of child fatalities (0 to 17 years) by county was analyzed for calendar year 2021 using
a crude rate. A crude rate is the number of cases (or deaths) occurring in a specified population per
year, usually expressed as the number of cases per 100,000 population at risk. Sierra County
exhibited the highest child fatality rate (11.1), followed by Quay (5.6), Sandoval (3.3), Torrence (3.2),
Otero (3.2), Curry (3.0), and Luna (2.9) county (Figure 9).
Source: NM Bureau of Vital Records and Health Statistics,
& New Mexico's Health Indicator Data & Statistics (last accessed: November 29, 2023)
Figure 9. Crude Rate of Child Fatalities, by County in New Mexico, 2021
24
2023 Report
Methodology
In 2022, 84 unique cases were reviewed by NM-CFR across its four panels. The NM-CFR 2023 Report
summarizes and analyzes information about these 84 injury-related deaths of NM infants, toddlers,
children, and youth under the age of 18. The report covers child fatalities resulting from injuries that
occurred between the years 2018 and 2022. Each fatality was carefully reviewed in the calendar year
2022.
The data presented in this report are descriptive and not inferential. No analysis was carried out to
determine correlations or associations between variables.
This report should not be used to compare changes over time to previous CFR reports published
by the NMDOH Oice of Injury and Violence Prevention.
Such a comparison would be inaccurate
because of the overlap in year of death.
Materials Reviewed
Cases are prepared for review when NM BVRHS sends death certificates of individuals under 18 years
of age who meet the criteria for inclusion into one of the review panels to the Oice of Injury and
Violence Prevention. If the child was born in NM, the birth certificate is also provided. The NM Oice of
the Medical Investigator (OMI)’s database is then utilized to obtain death summaries, any death
investigation notes, and any available autopsy and examination notes.
Documents providing context for the circumstances leading up to and involving the child’s death may
be gathered. Additional documents may include, but are not limited to state, local, and/or federal law
enforcement records, medical records, court records, school records, obituaries, news media, and
social media posts. To supplement the records gathered for the review, panelists from the NM
Children, Youth and Families Department (CYFD) and Comprehensive Addiction and Recovery Act
(CARA) Program aend panel meetings and are available to provide additional information on the
child and family’s social history, as well as circumstances around the death.

25
Panel Reviews
From January 1, 2022, through December 31, 2022, 84 unique child deaths were reviewed. The child
fatalities reviewed in 2022 comprised deaths that occurred from 2018 to 2022 (Table 4). While an
eort is made to review cases in a timely fashion, not all cases receive data in a timely manner. Some
cases are criminally prosecuted, and adjudication may be desired by the panel prior to review. For
these reasons, some cases are not reviewed until these criteria are met, which may be some years
later.
Table 4. Cases Reviewed by NM-CFR, by Year of Death in New Mexico, 2022
Year of Death
Number of reviewed cases
2018
2
2019
7
2020
29
2021
43
2022
3
Each of the 84 unique child deaths were reviewed by at least one of the four panels (Table 5).
Occasionally, some child death cases received a second review to gain additional perspective from
another panel, which yielded a total of 87 reviews in calendar year 2022. Database entry for the
reviewed cases was also completed in the National Fatality Review Case Reporting System.
Table 5. Cases Reviewed by NM-CFR, by Primary Panel of Review in New Mexico, 2022
Review Panel
Frequency
Percent
Child Abuse, Neglect or Homicide
12
13.8%
Sudden Unexpected Infant Death
35
40.2%
Youth Suicide
16
18.4%
Unintentional Injury
24
27.6%
Total
87
100%

26
Most Child Deaths Are Preventable
According to the National Center for Fatality Review and Prevention (NCFRP), a child's death is
considered preventable if there was a reasonable opportunity for an individual or the community to
take action that could have altered the circumstances leading to the child's death. Figure 10 shows
that out of 84 unique child fatalities analyzed in this report, NM-CFR determined that 67 deaths
(80%) could have been prevented, and 2 deaths (2%) couldn’t be prevented. In ten cases, there was
not information about preventability (12%), and NM-CFR could not determine from the information
gathered whether the child’s death was preventable in five cases (6%).
To determine preventability, NM-CFR panelists review all available information about a child fatality.
Circumstantial information about each case is carefully reviewed, and a robust discussion about risk
and protective factors informs the determination of preventability. Each panelist determines if a case
was able or unable to be prevented, and the final determination is determined by poll.
80%
2%
6%
12%
0
10
20
30
40
50
60
70
80
90
Yes No Undetermined Unknown
% Child Fatalities
Preventability
Figure 10. Child Fatalities Reviewed by NM-CFR by Preventability in New Mexico, 2022
Source: NCFRP, Last accessed: October 3, 2023

27
Figure 12. Child Fatalities Reviewed by NM-CFR, by Witness Distribution in New Mexico, 2022
Of the cases reviewed by NM-CFR in 2022, autopsies were performed on 63 (75%) cases. Panelists
agreed with the primary cause of death listed on the death certificate and pathology report on 72
(86%) cases. Out of the reviewed cases, a total of 71 investigations (85%) were carried out involving
deaths. Furthermore, in 61 cases (73%), the investigation was completed at the location where the
child's death took place. The local emergency number or 911 was called in 79 (94%) of the child
deaths. Out of the child deaths reviewed, resuscitation was attempted in 54 cases, accounting for
64% of the total; in 31 (57%), of these cases, the resuscitation was attempted by parents,
bystanders, friends, or other individuals before emergency medical services (EMS) arrived at the
scene (Figure 11).
Figure 11. Review Summary of Child Fatalities Reviewed by NM-CFR, in New Mexico, 2022
Source: NCFRP, Last accessed: October 3, 2023
Source: N CF RP, Last accessed: October 3, 2023
9
4
3
2
1
0 2 4 6 8 10
Parent
Acquiantances
Stranger
Other
Caretaker/Babysitter
# Child Fatlities
Witness

28
The distribution of witnesses in the cases that were reviewed by NM-CFR is shown in Figure 12. A
witness to the incident was available at 16 (19%) of the cases reviewed. Among all cases witnessed,
most common witnesses at the child’s scene of death were a parent (n=9, 56.3%), followed by non-
relative/acquaintances (n=4, 25%), stranger (n=3, 18.8%), caretaker/babysier (n=2, 12.5%) and
other (n=1, 6.3%).
Source: N CF RP, Last accessed: October 3, 2023
The report analyzed a total of 84 cases and found that the circumstances of the children's deaths
varied in terms of location. The child's home was the most frequent location for children's deaths,
accounting for 59 cases (70%). The second most common location was on or near a roadway, with
nine cases (11%) The other location of 32 cases (38%) where incidents occurred included: driveway,
other recreational location, other parking area, shed behind a residential home, hotel room, RV trailer,
and at another person’s home (Figure 13).
70%
11%
38%
0
10
20
30
40
50
60
70
80
Home Road Other
% Child Fatalities
Incident place
Figure 13. Child Fatalities Reviewed by NM-CFR, by Incident Places in New Mexico, 2022

29
Case Demographic Information
To investigate the distribution and occurrence of these child fatalities, the demographic information
of the cases, including age, gender, location, race, and ethnicity were also analyzed.
Child fatalities were higher in males (n=54, 64%) than females (n=30, 36%), as shown in Figure 14.
The only gender information available for case review was derived from death certificates, which does
not denote gender identity of the cases, a limitation of case review.
Male
Female
Source: N CF RP, Last accessed: October 3, 2023
Figure 14. Child Fatalities Reviewed by NM-CFR by Gender in New Mexico, 2022
36
64

30
Source: N CF RP, Last accessed: October 3, 2023
Figure 15 illustrates the paern of males outnumbering females distributed across the dierent age
categories. The age group with the most deaths was infants under the age of one (n=35, 41.6%). This
was followed by age group 15 to 17 (n=26, 30.9%), then age group 10 to 14 (n=10, 11.9%), age group 1
to 4 (n=7, 8.3%) and then age group 5 to 9 (n=6, 7.1%).
17
3
4
1
5
18
4
2
9
21
0
5
10
15
20
25
less than 1 1 to 4 5 to 9 10 to 14 15 to 17
# Child Fatalities
Age Group
Female Male
Figure 15. Child Fatalities Reviewed by NM-CFR, by Age and Gender in New Mexico, 2022

31
Source: N CF RP, Last accessed: October 3, 2023
Analysis of race and ethnic categorical distribution of reviewed cases found that 41 (49.4%) cases
were of Hispanic or Latino ethnicity. Twenty-five (30.1%) cases were non-Hispanic/Latino White.
Twelve (14.4%) cases were American Indian or Alaskan Native, four (4.8%) cases were Black or African
American, and one (1.2%) case was Asian or Pacific Islander (Figure 16).
The analysis also examined the location of death of cases reviewed in 2022, by county, to explore the
distribution of cases across NM. Of the cases reviewed in 2022, the highest number of child deaths
were found in Bernalillo County, with 23 cases (27.8%). Following that, seven cases (8.3%) were out
of Doña Ana County, and six cases (7.14%) were out of San Juan County.
12
1
4
25
41
1
0
5
10
15
20
25
30
35
40
45
American
Indian or
Alaskan
Native
Asian/Pacific
Islander or
Native HI
Black White Hispanic/
Latino
Unknown
# Child Fatalities
Race/Ethnicity
Figure 16. Child Fatalities Reviewed by NM-CFR, by Race and Ethnicity in New Mexico, 2022

32
Manner of Death
The NM-CFR reviewed the manner of death, the way in which a death occurs, across dierent
demographics. The most common manner of child death reviewed by the NM-CFR in 2022 was
unintentional injury (classified as accidental by the OMI) accounting for 39 cases (46%). This was
followed by suicide with 16 cases (19%), homicide with 12 cases (14%), undetermined with 14 cases
(17%), and natural causes with three cases (4%) (Figure 17).
Source: N CF R P, Last accessed: October 3, 2023
Figure 17. Child Fatalities Reviewed by NM-CFR, by Manner of Death in New Mexico, 2022
Natural, 4%

33
An analysis of cases reviewed in 2022 by manner of death and gender (Figure 18) illustrates that most
cases reviewed, across various manners, were male. Twenty-six (30.9%) male children died by
accident compared to the female death count of 13 (15.5%). The number of male suicides (n=15,
17.8%) was significantly greater than that of females (n=1, 1.2%). In cases of homicide, the number of
male fatalities (n=7, 8.3%) was found to be higher compared to the number of female fatalities (n=5,
5.9%).
Source: N CF R P, Last accessed: October 3, 2023
2
13
1
5
9
1
26
15
7
5
0
5
10
15
20
25
30
Natural Accident Suicide Homicide Undetermined
# Child Fatalities
Manner of Death
Female Male
Figure 18. Child Fatalities Reviewed by NM-CFR, by Manner of Death and Gender in New Mexico, 2022

34
Figure 19. Child Fatalities Reviewed by NM-CFR, by Manner of Death and Age in New Mexico, 2022
Among 84 unique cases reviewed, the most frequent manner found was unintentional, which was
present in all age groups. The unintentional death count was highest for infants, accounting for 17
cases (20.2%), followed by the 15 to 18 age group with 12 cases (14.3%). Suicide was highest in the 15
to 18 age group with nine cases (10.7%) followed by the 10 to 14 age group with seven cases (8.3%).
Homicide was greatest in the 15 to 18 age group, with five cases (5.9%) (Figure 19).
Source: N CF RP, Last accessed: October 3, 2023
3
17
5
3
2
12
7
9
2
2
2
1
5
13
1
0
5
10
15
20
25
30
35
40
less than 1 1 to 4 5 to 9 10 to 14 15 to 17
# Child Fatalities
Age Group
Natural Unintentional Suicide Homicide Undetermined

35
Figure 20 illustrates the causes and manners of death for cases reviewed in 2022. Of the 39
unintentional injury deaths, asphyxia was the leading cause, accounting for 18 deaths (21.4%). This
was followed by motor vehicle-related incidents, which caused nine deaths (10.7%). Other causes of
death included poisoning (n=4, 4.8%), drowning (n=3, 3.6%), and various other or unclassified
causes (n=1, 1.2%). Additionally, there was one death each resulting from fall/crush,
fire/burn/electrical incidents, and bodily force or weapon use, each accounting for 1.2% of the total
deaths. Of the 16 suicide cases, nine (10.7%) were aributed to bodily force or weapon, while seven
(8.3%) were classified as asphyxia.
Source: N CF R P, Last accessed: October 3, 2023
1
9
1
3
18
1
1
4
1
7
9
3
12
13
1
0 10 20 30
Unknown
Motor Vehicle
Fire, burn or electrocution
Drowning
Asphyxia
Bodily force or weapon
Fall or crush
Poisoning, overdose or acute intox
Other
# Child Fatalities
Causes of Death
Unintentional Suicide Natural Homicide Undetermined
Figure 20. Child Fatalities Reviewed by NM-CFR, by Cause and Manner of Death in New Mexico, 2022

36
Child Abuse, Neglect or Homicide (CAN-H)
In 2022, 12 child fatalities were reviewed by the CAN-H Panel, each of which was a unique case. Of the
12 cases of child abuse, neglect, or homicide included in this report, eight (66.7%) were males, and
four (33.3%) were female. Eight (66.7%) of the children were Hispanic or Latino, three (25%) children
were White, one (8.3%) child was Black or African American. Out of 12 cases reviewed in this panel, six
cases (50%) were reported in the age group of 15 to 17 years. There were two cases (16.6%) each in
the age group of one to four years and five to nine years. Additionally, there was one case (8.3%) in
each age group of less than one year and 10 to 14 years (Figure 21).
Source: N CF R P, Last accessed: October 3, 2023
Gender
Age
Race & E t h n ic it y
4
8
1
2 2
1
6
1
3
8
0
1
2
3
4
5
6
7
8
9
# Child Fatalities
Age
Race & Ethnicity
Gender
Figure 21. Child Fatalities Reviewed by NM-CFR (CAN-H panel) by Demographics in New Mexico, 2022
37
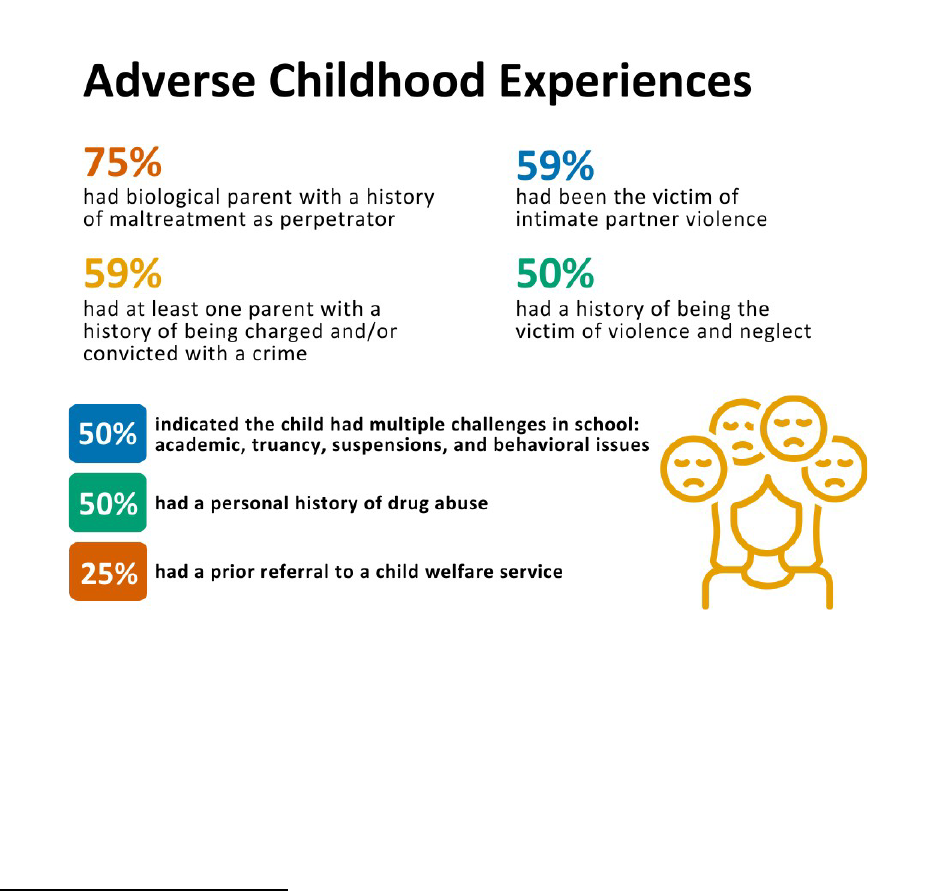
Of the 12 child fatality cases reviewed in CAN-H panel in 2022, 75% (n= 9) were identified as
having a history of maltreatment with a parent as a perpetrator. A quarter of children (n=3,
25%) had a prior referral to child welfare services. More than half of the children (n=7, 59%)
had at least one parent with a history of being charged and/or convicted of a crime.
Half of the children (n=6, 50%) had a history of victimization of violence or neglect, had a
personal history of substance misuse, or faced multiple challenges in school such as
academics, truancy, suspensions, or behavioral issues. Seven (59%) children were also
victims of intimate partner violence (Figure 22).
Source: NCFRP, Last accessed: October 3, 2023
The socioeconomic background
2
of six (50%) of these 12 children was categorized as low,
while the economic background of the remaining six cases reviewed was unknown. The
evaluations of these fatalities brought aention to several risk factors, one of which was the
presence of notable Adverse Childhood Experiences (refer to the Shared Risk and Protective
Factors for Child Fatality in NM section, page 45).
2
According to the National Center for Fatality Review and Prevention, “Income level is an estimate
based on economic indicators such as caregiver education, social service enrollment, and health
insurance type; can assist in determining the child’s household income level. If no concrete evidence
exists regarding income, unknown is selected” (NCFRP, 2022).
Figure 22. Summary of Adverse Childhood Experiences in Child Fatalities Reviewed by NMCFR (CAN-H panel) in
New Mexico, 2022

38
Sudden Unexpected Infant Death (SUID)
Sudden unexpected infant death (SUID) is a term used to describe the sudden and
unexpected death of a baby less than one year old in which the cause was not obvious
before investigation. These deaths often occur during sleep or in the area where the infant
was placed to sleep.
Three commonly reported types of SUID include: sudden infant death syndrome (SIDS),
accidental suocation and strangulation in bed and unknown cause.
In 2022, 34 reviews of infant fatalities were conducted by the Sudden Unexpected Infant
Death (SUID) Panel. One case was reviewed twice by this panel. Three were ultimately
excluded from final analysis as the case characteristics did not meet inclusion criteria for the
Centers for Disease Control and Prevention’s SUID Case Registry. The three excluded cases
are described further in the Exclusions subsection. More information about the SUID Case
Registry can be found at hps://www.cdc.gov/sids/case-registry.htm
Of the 30 unique cases which met inclusion criteria and were analyzed in this report, 16
(53.3%) were male and 14 (46.7%) were female, 14 (46.7%) were Hispanic or Latino, nine
(30%) were White, five (16.7%) were Native American, and two (6.7%) were Black or African
American. In terms of age, most were between 1-8 months of age. Three (10%) were less
than one month old, and one (3.3%) was more than nine months old. Table 6 displays counts
and percentages of cases by age.
Table 6. Child Fatalities Reviewed by NM-CFR (SUID Panel) by Age Group in New Mexico, 2022
Age
Count
Percent
Sudden unexpected early neonatal deaths (SUEND), 0-6 days of life
0-6 days old
0
0%
Post-perinatal SUID, 7-364 days of life
< 1 month old
3
10%
1-4 months old
13
43.3%
5-8 months old
13
43.3%
9-12 months old
1
3.3%
Total
30
100%
Selected Risk Factors for SUID
Sleep and caregiver characteristics such as infant sleep position, surface and location which
increase the risk of SUID, as well as exposures and other risk factors, are described in the
2022 AAP Technical Report on SUID
(Moon, et al. 2023).

39
Of note, while surface sharing (adult or other person sleeping on the same surface, such as
adult bed, couch, recliner or futon) alone poses an increased risk of SUID, some additional
characteristics significantly increase the risk of accidental strangulation or suocation in
bed and wedging or entrapment. Bed sharing with someone who is impaired in their alertness
or ability to arouse because of fatigue or use of sedating medications (e.g., certain
antidepressants, pain medications) or substances (e.g., alcohol, illicit drugs), bed sharing
with a current smoker (even if the smoker does not smoke in bed) or smoking during
pregnancy can increase the risk of SUID by more than 10 times the baseline risk of parent-
infant bed sharing.
The following sections describe characteristics of NM SUID cases reviewed by NM-CFR in
2022:
Sleeping environment and place
In 20 cases (67%), the death was identified as related to an unsafe sleep environment. In
three cases, the infant was placed to sleep in a bassinet and in another two cases, the infant
was placed to sleep in a crib (Figure 23). Although cribs and bassinets meet
safe sleep
recommendations, the presence of other items are not recommended. Items such as soft
objects, like pillows, pillow-like toys, quilts, comforters, maress toppers, fur-like materials,
and loose bedding (blankets and nonfied sheets) increase the risk of suocation,
entrapment/wedging, and strangulation.
In fifteen (50%) cases, the infant was placed to sleep on an adult bed. In 17 cases (57%), the
infant was placed to sleep sharing a sleep surface with another person or animal. Of the 17
cases related to surface sharing, eight (27%) were noted to have no infant crib or safe sleep
space in the home. In one case (3%), the family was noted to be experiencing housing
insecurity and/or homelessness.
Source: N CF R P, Last accessed: October 3, 2023
2
3
15
1
3
1
0
2
4
6
8
10
12
14
16
Crib Bassinet Adult bed Couch Other Futon
# SUID cases
Sleeping place
Figure 23. Child Fatalities Reviewed by NM-CFR (SUID Panel), by Sleeping Place in New Mexico, 2022
40
Caregiver Impairment
Caregiver impairment is defined broadly by the NCFRP and includes being distracted or
absent, impaired by illness or disability, and impaired by substances such as medications,
alcohol or other substances.
An analysis of adult caregivers who were intoxicated by alcohol, medication or other
substances (prescribed or illicit) at the time of the incident was conducted. Of the 30 unique
SUID cases reviewed in 2022, six cases (20%) in which the adult caregiver was impaired were
identified, which may be an underrepresentation of the actual proportion. There were five
cases (17%) identified in which the adult caregiver was intoxicated by alcohol, and one (3%)
in which the adult caregiver was impaired by other substances.
SUID Categorization
Cases were categorized using the CDC SUID Registry Case Categorization Algorithm. Of the
30 unique cases reviewed in 2022, 13 (43%) were categorized as explained and determined
to be due to suocation with unsafe sleep factors; 11 (37%) were categorized as unexplained
with unsafe sleep factors present; two cases (7%) were categorized as unexplained,
possible suocation with unsafe sleep factors present and one case (3%) was categorized
as unexplained due to incomplete case information available.
Primary Mechanism of Injury
The primary mechanism of injury in eight cases (27%) was identified as soft bedding. In six
cases (20%), the primary mechanism of injury was overlay, and in one case (3%), it was
wedging.
Exclusions
Out of the 34 cases reviewed by the SUID panel, three cases were ultimately excluded
because they did not meet the criteria for SUID as described by the CDC, as their cause of
death was determined to be natural. Two (66.6%) of these cases were female and one
(33.3%) was male. All three were Hispanic or Latino. Among them, two cases fall into the one
to four months age category, while one case falls into the five to eight months age category.

41
Unintentional Injury
Unintentional injuries can be caused by poisoning, inhalation or ingestion, motor vehicle
crashes, falls, drowning, and structural fire or thermal injuries, firearms, or other
mechanisms. In 2022, 24 unique child fatalities were reviewed by the Unintentional Injury
Panel. Twelve (50%) of the cases reviewed were of children 15-17 years old (Figure 24).
Twenty-three cases (96%) were identified as preventable; only one (4%) case was identified
not to be preventable. Fifteen (62%) cases were males, and nine (37.5%) cases were female.
Twelve (50%) of the 24 children were Hispanic or Latino, five (20.8%) of which identified as
White, and six (25%) were Native American. The leading causes were asphyxiation (n=11,
46%), motor vehicle crashes (n=6, 25%), poisoning (n=3, 13%), falls (n=1, 4%), drowning
(n=1, 4%), bodily force or weapon (n=1, 4%), and other incidents (n=1, 4%).
Source: N CF R P, Last accessed: October 3, 2023
1
5
4
2
12
0
2
4
6
8
10
12
14
less than 1 1 to 4 5 to 9 10 to 14 15 to 17
# Unintentional Injury
Age Group
Figure 24. Child Fatalities Reviewed by NM-CFR (Unintentional Injury Panel), by Age Group in New Mexico, 2022

42
Youth Suicide
Of the 16 unique cases of child suicide included in this report, fifteen (93.8%) were males and
one (6.3%) was female. Nine (60%) were white, four (26.7%) were Hispanic or Latino. Of the
reviewed cases, nine (56%) were in the 15 to 17 age group and seven (44%) were in the 10 to
14 age group (Figure 25).
Fifteen (93.8%) of the cases were identified as preventable by the NM-CFR; the team could
not determine preventability for one (6.3%) case.
10 to 14
15 to 17
Source: N CF RP, Last accessed: October 3, 2023
Mental Health Status and Suicide Ideation
Of the youth suicide cases reviewed in 2022, fourteen (88%) were identified as having
experienced a sense of isolation. Eleven (69%) had experienced a major life stressor or crisis
within the 30 days before their death. Prior to their death, seven (44%) children had
communicated thoughts or intention of suicide to someone else, and 69% had a history of
self- harm. Four (25%) experienced a change in behavior prior to their death. Three (19%)
were diagnosed with depression; two (13%) were diagnosed with anxiety. Two cases (13%)
had previously aempted suicide, yet none of the records reviewed indicated that a safety
plan was in place at the time of their death.
Figure 25. Child Fatalities Reviewed by NM-CFR (Suicide Panel), by Age in New Mexico, 2022
44
56

43
Half of the children (n=8, 50%) that died by suicide had received prior mental health
services. Six (37.5%) were actively receiving mental health services around the time of
death. Two (12.5%) children had been seen in the emergency department for a mental health
emergency within the last 12 months; however, no information was found about follow-up
appointments within 30 days.
Social Characteristics
Of the youth suicide cases reviewed in 2022, half (n=8, 50%) had parents who were divorced
or separated. Before their death, six (38%) had recently argued with their parents,
experienced a life stressor in terms of failure in school, or had been raised in a home with
domestic violence. Four (25%) had experienced housing insecurity; four (25%) had been the
victim of bullying. Two (13%) had experienced the death of a loved one, and two (13%) had
recently gone through a breakup with a significant other.
Figure 26. Summary of Suicide Ideation, Behavioral and Mental Health Status of Child Fatalities Reviewed by
NM-CFR (Suicide Panel), in New Mexico, 2022

44
Source: N CF R P, Last accessed: October 3, 2023
Figure 27. Summary of Stressful Events related to Child Fatalities Reviewed by NM-CFR (Suicide Panel), in New
Mexico, 2022

45
Shared Risk and Protective Factors for Child Fatality in NM
In this analysis, some themes about risk and protective factors emerged across the review
panels:
Life Stressors & Mental Health as a Risk Factor for Child Fatality
Through the cases reviewed in 2022, some shared risk factors were identified: life stressors
such as failure in school, death of a loved one, argument with parents, bullying, parents
divorced/separated, recent breakups, and mental health challenges (thoughts or intentions
of suicide, depression or anxiety, self-harm, prior suicide aempt).
Lack of Mental Health Services as Risk Factors
According to the National Alliance on Mental Illness (NAMI), New Mexicans are 1.5 times more
likely to be forced out-of-network for mental health care than for primary health care. More
than 59% of New Mexicans aged 12–17 who have depression did not receive any care in the
last year.
In the analysis of youth suicide cases reviewed, four (25%) of 16 cases were identified as
having several issues leading to non-utilization or underutilization of mental health services.
These issues included: lack of providers in rural areas, refusal of parents or child to
participate or utilize referrals, stigmas around mental health or about receiving mental health
supportive services, and travel distance to services.
Access to Lethal Means as a Risk Factor for Child Fatality
Access to lethal means such as firearms, medication and other instruments or objects which
may result in intentional injury increases the risk of death by homicide and suicide, as well as
other unintentional injuries such as accidental gun deaths and accidental overdose.
Eighteen percent (n=15, 17.8%) of all 84 cases reviewed in 2022 were due to firearm injury.
Nine (56%) suicide deaths were due to firearm injury. Five (41.7%) of the 12 cases reviewed by
the CAN-H panel were due to firearm injury. One unintentional injury death reviewed in 2022
was by firearm. Four (16.7%) cases reviewed by the Unintentional Injury panel were due to
accidental overdose.
A 2023 report by the NMDOH
, Comprehensive Report on Gunshot Victims Presenting at
Hospitals in New Mexico, identified lack of safe storage as risk factor for firearm injury and
death. Reducing access to lethal means through safe storage of firearms and medication
could save lives in the future.
46
Lack of Supervision as a Risk Factor for Child Fatality
According to the NCFRP, lack of supervision is defined as a child who did not have supervision
but needed it, with children less than age six requiring constant supervision most of the
time. In addition, if the supervisor of a child younger than age six could not see or hear the
child at the time of need, this would be considered lack of supervision.
For the 84 children included in this report, at the time of the incident which led to the child’s
death, less than half of children (n=38, 45.2%) were supervised at the time of death and 17
children (20.2%) did not have supervision and needed it. In 15 (17.9%) cases, the child who
died was of suicient developmental age and circumstances to supervise themselves. In one
case, the NM-CFR was not able to determine the child’s supervisory need. Thirteen (15%)
cases did not have any response entered in the database.
Regardless of supervision status at time of incident leading to death, 38 of the 84 (45%)
cases analyzed contained information about the last time a primary person responsible for
supervision at time of incident saw the child: in 26 (30.5%) of those cases, the deaths
occurred when the child was in sight of the supervising individual; two deaths (2.3%)
occurred when the child was out of sight of the supervising individual for less than an hour;
nine deaths (10.7%) occurred when the child was out of sight of the supervising individual for
more than an hour.
A range of risk factors were identified from the available records of 55 children who were
noted as needing supervision or who were under parents/caregiver(s) supervision at the
time of their death. In 21 (38.1%) cases, the individual responsible for supervising the child
was asleep at the time of the child’s death. Seventeen children (30.9%) were supervised by
an individual who had a known history of child maltreatment. Thirteen children (23.6%) were
supervised by an individual with a known history of substance use disorder. Ten children
(18.2%) were supervised by an individual who was convicted of a crime. Nine children (16.3%)
were supervised by an individual who had a history of intimate partner violence victimization.
Six (10.9%) child deaths occurred in situations where the supervising adult was impaired
(defined by the NCFRP as being “distracted or absent, drug or alcohol impaired, and/or
impaired by disease or disability”). Five (9%) child deaths occurred in situations where the
supervising individual had a disability or chronic illness.
Adverse Childhood Experiences as a Risk Factor for Child Fatality
NM Behavioral Risk Factors Surveillance System data indicate that an estimated 68% of
adults residing in NM experienced at least one ACE, and nearly one in four (23.8%)
experienced four or more ACEs (Whiteside, 2021). As a person’s number of ACEs increases,
so does the risk for negative health and life outcomes.
Among the 84 cases reviewed in 2022, 30 children (35.7%) had a history of maltreatment
with a perpetrator parent. Eighteen children (21.4%) had lived with at least one parent who

47
was convicted of a crime. A history of referral to child welfare services was found in 10 cases
(12.4%). Thirteen children (15.5%) experienced multiple challenges in school such as
academics, truancy, suspension, or behavioral issues. Eighteen (21.4%) had history of
intimate partner violence, and 19 (22.6%) had history of substance misuse.
Child Maltreatment & Child Health as Risk Factors for Child Fatality
A history of child maltreatment has been identified as a risk factor for preventable child
fatality (Jonson-Reed, et al., 2022). Twenty-seven (32.1%) of the 84 cases reviewed by NM-
CFR in 2022 had a history of child maltreatment, and four (4.7%) had open investigations at
the time of their death. Eight children (9.5%) had a history of being placed into foster care at
any time prior to their death.
Child health status can also be a stressor for families that increases the risk of child fatality.
Twenty-one (25%) children had a known prior disability or chronic illness. Nine children
(10.7%) were receiving mental health services prior to their death and another 15 children
(17.9%) had received mental health services in the past. Nineteen children (22.6%) had a
history of substance use prior to their death.
Socioeconomic Status (SES) as a Risk Factor for Child Fatality
Social determinants of health, the conditions in which people live, work and play, have a
significant eect on health and well-being. Socioeconomic status (SES) is a notable finding
in this analysis. Two children (2.4%) were classified as having high household income, 11
children (13.1%) were classified as having medium household income, 30 cases (35.7%) were
classified as having low household income, and 29 (34.5%) cases were unknown or unable to
classify.
Health insurance information gives further insight into the SES of these children. A
2021
factsheet by NAMI indicated that 9.8% of people in NM are uninsured. In the analysis of
insurance status for the 84 unique child fatalities reviewed by NM-CFR in 2022, 48 cases
(57.1%) had Medicaid as their insurance coverage, 30 cases (35.1%) had private insurance
coverage, and one child (1.2 %) had no medical coverage. Twenty-two (26.2%) case records
indicate that their mothers received prenatal care, a known preventive factor of child fatality.
In the cases reviewed and analyzed in this report, social determinants such as household
income, geographic location, or education level may have prevented these children or their
parents/caregivers from equitable access to and use of healthcare services.
48
Limitations
A limitation of this report is that data were missing for several variables. During the
comprehensive review of these cases, certain information was unavailable due to various
factors, such as records requests which were not received by the agency. In cases where
there were diiculties in accessing data, it was necessary to classify certain values as
'unknown'. This lack of comprehensive data may contribute to underrepresentation of some
variables in this report.
Conclusions
Child deaths due to injury and violence are predictable and preventable. Of the unique 84
child fatalities reviewed in 2022 and described in this report, NM-CFR determined that 67
(79.76%) deaths could have been prevented. In most cases, there was suicient data for the
NM-CFR to determine preventability, however, in five (5.6%) cases, the information provided
was insuicient to determine whether the child’s death was preventable. Based on child
fatality data from reviews conducted during calendar year 2022 and analyzed in this report,
the leading causes of death were: asphyxiation (30%), bodily force or weapon (27%),
unknown (20%), and motor vehicle crashes (11%), followed by poisoning (5%), drowning
(3%), and other incidents (3%). The most common circumstances surrounding child deaths
in NM included risk factors and a lack of protective factors in areas of access to lethal means,
behavioral and mental health care, supervision, income level in family, maltreatment, and
violence.
A broad evidence base demonstrates that social determinants of health, such as educational
aainment, economic stability, social and community dynamics, neighborhood
characteristics, and access to quality healthcare, as well as discriminatory policies, systemic
violence and historical trauma contribute to the manifestation of complex and
interconnected risk factors for children and families. Enacting preventative measures can
reduce risk factors such as adverse childhood experiences, mitigating trauma and creating a
protective environment to reduce the occurrence of child fatalities.
Recommendations to prevent adverse childhood experiences and promote positive
childhood experiences to increase protective factors include strengthening economic
supports for families; promoting social norms that protect against violence and adversity;
ensuring a strong start for children; teaching skills; connecting youth to caring adults and
activities; and intervening to lessen immediate and long-term harms.
The next section describes key prevention recommendations made by NM-CFR.

49
NM-CFR Recommendations
Previous Recommendations
Although some recommendations from previous years have not yet been implemented, and
may not be included in this report, the NM-CFR recognizes the continued need for adoption.
Exclusion from this report should not be interpreted as a discontinued need. The key
recommendations were selected and included in this report based on current public health
and social conditions, as well as alignment with departmental priorities.
Some recommendations that were made by NM-CFR panelists in 2022 have since been
implemented, and thus excluded from the Key Recommendations. The following actions have
been taken based on previous recommendations of the NM-CFR:
A long-standing infant injury prevention recommendation of the NM-CFR included shaken
baby syndrome (SBS) prevention. In 2017, the Shaken Baby Syndrome Educational Materials
Act was enacted in NM, which requires hospitals and freestanding birth centers to provide
training and education to prevent SBS to every parent of every newborn before discharge.
One recommendation made in 2022 was for the NM-CFR to develop a panel to address
violence aecting youth, oftentimes, but not limited to causes by firearm injury. In 2023, the
NM-CFR created a new panel to review cases related to community and/or peer violence.
Another recommendation which was made in previous years as well as in 2022 was for a
legislative mandate for the safe storage of firearms in homes with children. In 2023,
House
Bill 9, the Bennie Hargrove Gun Safety Act was enacted, which prevents gun violence by
requiring gun owners to keep firearms safely stored.
A recommendation that funds be appropriated for Sudden Unexpected Infant Death
Education and Prevention, including funding for the purchase and provision of safe sleep
spaces such as bassinets and cribs, was realized in 2023 when the Early Childhood,
Education and Care Department (ECECD) was allocated funds for safe sleep in the Thriving
Families Prenatal to Three (PN-3) Prevention Plan. However, recurring funding is needed to
sustain these activities.
50
Discussion of Recommendations
Qualitative assessment and analysis of responses by NM-CFR panelists across its four
panels revealed themes related to safe infant sleep, firearm safety and storage, motor
vehicle and pedestrian safety, and behavioral health care, including mental health and
substance use needs.
NM-CFR panelists highlighted significant challenges faced by children and families, including
poverty, lack of access, or barriers to engagement with social services, trauma informed and
culturally appropriate care:
“When a high count of CYFD reports [and] refusal of help by family, this is a sign of
high-risk of abuse and neglect.”
NM-CFR CAN-H Panelist
“Resources for culturally sensitive safe sleep education for parents that reside on
tribal land.”
NM-CFR SUID Panelist
The key recommendations included in the next section include recommendations to
strengthen the NM-Child Fatality Review for improved data and recommendations for
preventing child deaths, recommendations to increase safe home environments and
recommendations to increase behavioral healthcare and access to resources.
With regard to the recommendations to strengthen the NM-Child Fatality Review for
improved data and recommendations for preventing child deaths, the NM-CFR was created
with the passing of an unfunded mandate. At the time of publication of the first NM-CFR
Annual Report in 2000, NM-CFR sta consisted of one full-time equivalent (FTE)
Epidemiologist and one 0.5 FTE Coordinator. Currently, the statewide program is operated by
1.0 FTE, the Child Fatality Review Coordinator, of which the salary is funded through state
general funds. To date, there is no budget to support program operations, such as data
collection and management, nor for salaries, oice supplies, or other items. Recurring
funding to support program operations would improve program capacity. Dissemination of
this report as well as other publications by NM-CFR or the Oice of Injury & Violence
Prevention would increase awareness of the program, increase statewide knowledge of
prevention recommendations, and may contribute to increases in prevention programming
and coordination across sectors to prevent child fatalities in NM.

51
Key Recommendations
Recommendations to strengthen the NM-Child Fatality Review for improved data and
recommendations for preventing child deaths:
1. The NM Legislature should appropriate recurring funding to support the NM Child
Fatality Review in its programmatic operations and activities.
2. State agencies, NM-CFR Panelists, policymakers, the media, and the public should
disseminate this report and its findings widely, in remembrance of those it describes,
and to increase awareness of the burden of child fatality in New Mexico, as well as
prevention eorts.
Recommendations to increase safe home environments:
3. The NM Legislature should pass legislation that requires hospitals, birthing facilities,
midwives and birth workers to provide education to parents and caregivers about safe
infant sleep practices, as prescribed by the American Academy of Pediatrics, and
training for appropriate personnel in state-funded infant-serving organizations,
including childcare facilities and departments such as the Early Childhood, Education
and Care Department and the Children, Youth and Families Department.
4. Child-serving agencies and organizations should implement policy and make available
resources to improve safe home environments for families, such as gun locks, baby
gates and products to encourage safe infant sleep practices, smoke and carbon
monoxide detectors and airway clearing devices.
Recommendations to increase behavioral healthcare and access to resources:
5. The NM Legislature should pass legislation that provides increased access to mental
health professionals from other states via telehealth by joining a multistate compact
such as Psychology Interjurisdictional Compact (PSYPACT), an interstate agreement
which allows psychologists in participating jurisdictions to practice across state lines
and includes provisions for tele-practice.
6. The Children, Youth and Families Department, Early Childhood, Education and Care
Department, Department of Health, and Public Education Department should require
suicide prevention gatekeeper training, such as QPR (Question. Persuade. Refer.™
) or
Mental Health First Aid for appropriate personnel. These trainings are also
recommended for personnel in state-funded child-serving organizations, including
public schools, behavioral health care seings, medical and childcare seings (i.e.
YMCA, Boys and Girls Club etc.).
7. The NM-CFR supports the implementation of a centralized reporting and referral
database that can be utilized by state agencies, police departments, medical
providers, and other partners to flag and assist children who are being exposed to
violence and need referrals, especially mental health.

52
Appendix
Appendix A: Acknowledgements
The NMDOH would like to express appreciation to all the members of the 2022 NM-CFR
panels: Child Abuse, Neglect or Homicide, Sudden Unexpected Infant Death, Unintentional
Injury and Youth Suicide. Individuals on these panels include state and local experts in
diverse fields as well as occasional aendees brought to specific case reviews. Thank you for
your dedicated time, expertise, and feedback to aid in reducing child fatalities and injuries in
New Mexico.
Name
Organization
Abby Turner
Western New Mexico University
Aidan Kerr
Oice of the Medical Investigator
Alberto Aldana
Roswell Police Department
Alexis Grasse
Guest
Alina Potrzebowski
Department of Health
Allie Heredia
Bernalillo County Sheri’s Oice
Anelle Brand
Oice of the Medical Investigator
Angela Baca
Children, Youth and Families Department
Arthur Malone
Pojoaque Pueblo Social Services
Ashley Anaya
Children, Youth and Families Department
Barbara Salazar
Children, Youth and Families Department
Bella White
Breaking the Silence NM
Benjamin Vickers
Department of Health
Benny Chen
University of New Mexico Hospital
Catherine Small
Bernalillo County Sheri’s Oice
Chloe Stoel
University of New Mexico Hospital
Christopher Trujillo
Department of Health
CL Kieer Nail
Department of Health
Clarie Miller
Department of Health
Clarissa Krinsky
Oice of the Medical Investigator
Colinda Vallo
Children, Youth and Families Department
Ross Daugherty
Bernalillo County Sheri's Department
Doug Parson
Chaves County CASA
Dylan Pell
Department of Health
Edith Lewis
Children, Youth and Families Department
Erika Myers
University of New Mexico Hospital
Fahad Hussain
University of New Mexico Hospital
Garry Kelly
Department of Health
Harley Schainost
Oice of the Medical Investigator
Hayley Peterson
Department of Health
Heather Carrica
Children, Youth and Families Department
53
Holly Burks
Department of Health
Jacalyn Dougherty
Department of Health
Jeanne Masterson
Children, Youth and Families Department
Jerey Bullard-Berent
University of New Mexico Hospital
Jennifer Hart
Albuquerque Public Schools
Jennifer Padge-Macias
Santa Fe County District Aorney’s Oice
Jessi Fuchs
Department of Health
Jimmy Gibson
Public Education Department
Joshua Lopez
University of New Mexico/Albuquerque Ambulance Service
Karen Campbell
University of New Mexico Hospital/Children, Youth and
Families Department
Katherine Schafer
University of New Mexico
Kathleen Maese
Department of Health
Kathryn Lowerre
Department of Health
Keisuke Abe
University of New Mexico
Kelly Hynes
Oice of the Medical Investigator
Kimberly Prue
University of New Mexico
Kylie Diver
Children, Youth and Families Department
Laura Geiger
University of New Mexico Hospital
Laura Migliaccio
University of New Mexico Hospital
Lauren Dvorscak
Oice of the Medical Investigator
Leslie Kelly
Public Education Department
Leslie Strickler
University of New Mexico Hospital
Lidia Bachechi
Children, Youth and Families Department
Lisa Rohleder
Children, Youth and Families Department
Liza Suzanne
Department of Health
Lori Proe
Oice of the Medical Investigator
Lori Zigich
Oice of the Medical Investigator
Lucretia Vigil
Department of Health
Maggie Edmiston
Cibola Hospital
Maryanne Chavez
University of New Mexico Hospital and Para Los Niños
Ma Cole
City of Santa Fe
Melissa Ewer
NM Coalition of Sexual Assault Programs
Mercedes Barr
Children, Youth and Families Department
Michael Harrell
Oice of the Medical Investigator
Natasha Sing
Chaves County CASA/Child Advocacy Center
Nicholas Marshall
United States Aorney’s Oice – District of NM
Nicholas Sharp
Department of Health
Nicole Urrea
University of New Mexico Hospital
Rachel Ralya
Department of Health
Rachel Wexler
Department of Health

54
Rebecca Girardet
University of New Mexico Hospital
Rebecca Tarin
Oice of the Medical Investigator
Ronaldo Chavira
Court Appointed Special Advocate
Ruth Golar
Albuquerque Public Schools
Samantha Medeiros
Department of Health
Sarah Johnson
Chaves County CASA/Child Advocacy Center
Sco Paerson
Administrative Oice of the Courts
Sean Thomas
Albuquerque Public Schools
Shayna Klassen
Department of Health
Shelly Bucher
Substitute Care Advisory Council
Sophie Rodriguez
Oice of the Medical Investigator
Stephanie McGovern
University of New Mexico Hospital
Susan Merrill
Department of Health
Teri Coer
Department of Health
Theresa Yazzie
Indian Health Service
Toby Rosenbla
Department of Health
Travis Hardy
Chaves County Sheri Oice
Wendy Linebrink-Allison
NM Crisis and Access Line
Special thanks to outgoing panelists Angela Baca, Mercedes Barr, Heather Carrica, Kylie
Diver, Jacalyn Dougherty, Jessi Fuchs, Michael Harrell, Garry Kelly, Nadja Maia, Laura
Migliaccio, Mishka Moncriee, CL Kieer Nail, Alina Potrzebowski, Lori Proe, Nicholas Sharp,
Toby Rosenbla, Rebecca Tarin, Colinda Vallo and Benjamin Vickers for their dedication to
Child Fatality Review and Prevention in New Mexico.
Appreciation and thanks are extended to the sta at the New Mexico Oice of the Medical
Investigator, New Mexico Children Youth and Families Department, the New Mexico Bureau of
Vital Records and Health Statistics (BVRHS), state and federal law enforcement agencies,
medical facilities, and school districts across New Mexico who aided in supplying much
needed data for the case reviews included in this report.
Warm appreciation also to colleagues who contributed to this report: Naja Druva, Samantha
Medeiros, Susan Merrill, Clarie Miller, Mishka Moncriee, Dylan Pell, Jennifer Schusterman,
Richard Spano, Liza Suzanne, and Desiree Valdez.
Most of all, we would like to acknowledge the families, friends and communities aected by
child loss in our state. It is with deepest sympathy that we dedicate this report to the
children represented in its pages.
NM-CFR welcomes commied individuals to participate in one or more of the review panels.
Those with experience in the fields of mental health, family-focused social services,
substance abuse, early childhood services, law enforcement, criminal justice, transportation
safety, faith-based initiatives, emergency medical services, and school-based health
services are especially encouraged to participate. To get involved, please contact
NMCFR@doh.nm.gov
.

55
Appendix B: State of New Mexico Child Death Review Legislation
As outlined in 7 NMAC 4.5, which can be found at hps://www.ncfrp.org/wp-
content/uploads/State-Docs/NM_leg.pdf, the New Mexico Department of Health has the
regulatory authority to operate a child fatality review program. The Department of Health Act,
Section 9-7-6. E. NMSA 1978 and the Public Health Act, Section 24-1-3. F NMSA 1978
specifically, states “The department has authority to: investigate, control and abate the
causes of disease, especially epidemics, sources of mortality and other conditions of public
health; and Section 24-1-3. F. NMSA 1978, which states: “The department has authority to:
establish programs and adopt regulations to prevent infant mortality, birth defects and
morbidity”.
7.4.5.2 thru 7.4.5.15 in Title 7 outline this statutory authority as well as the program
administration, oversight, membership, case identification, data collection, confidentiality
and security of records, proceedings, and findings.

56
Appendix C: Glossary Terms from OMI 2021 Annual Report
Cause of Death
“The agent of effect that results in a physiological derangement or
biochemical disturbance that is incompatible with life. The results
of postmortem examination, including autopsy and toxicological
findings, combined with information about the medical history of
the decedent serves to establish the cause of death. The cause of
death can result from different circumstances and manner of
death. For example, the same cause of death, drowning, can result
from the accidental immersion of a child in a swimming pool or from
the homicidal immersion of a child in a bathtub.”
Manner of Death
“The general category of the condition, circumstances or event,
which causes the death. The categories are natural, accident,
homicide, suicide and undetermined.”
Natural
“The manner of death used when solely a disease causes death. If
death is hastened by an injury, the manner of death is not
considered natural.”
Accident
“The manner of death used when, in other than natural deaths,
there is no evidence of intent.”
Homicide
“The manner of death in which death results from the intentional
harm of one person by another.”
Suicide
The manner of death which results from intentional self-injury.
Undetermined
“The manner of death for deaths in which there is insufficient
information to assign another manner.”
Pending
“The cause of death and manner of death are to be determined
pending further investigation and/or toxicological, histological
and/or neuropathological testing at the time of publication”
57
Appendix D: Oice of the Medical Investigator Annual Report 2021 –
Excerpt (page 44)
Deaths of Children in New Mexico – Summary
The 10-year summaries presented in this report for childhood deaths all include ages 19 and
younger. The 361 deaths of people aged 19 and younger represented 3.51% of all deaths
investigated by the OMI in 2021. Male decedents comprised 58.27% of the total deaths in
children. The most common manner of death among children was natural, contributing
21.95% of the total. There were 32 suicides among children in 2021. Suicide deaths were more
common among young males (78.12%) than females (21.88%). The total number of childhood
homicides increased from 24 homicides in 2020 to 29 in 2021. Homicide deaths among
children tended to be male (82.76%), White Hispanic/Latino (44.83%). The majority of
childhood homicide victims (68.97%) were between the ages of 15 and 19. Homicide rates
increased by 20.83% from 2020 to 2021 with the largest homicide population impacting the
age group 15–19 years.

58
Appendix E: Suicide Awareness, Prevention and Training Organizations
Breaking the Silence New Mexico hp://www.breakingthesilencenm.org
Campaign Against Living Miserably (CALM) hps://www.thecalmzone.net
Child Mind Institute hps://childmind.org/topics/trauma-grief
Coalition to Support Grieving Students hps://grievingstudents.org
Herald Alliance, The K-12 Toolkit for Mental Health Promotion and Suicide Prevention
hp://www.heardalliance.org/wp-content/uploads/HEARDToolkit2017.pdf
Mental Health America hps://mhanational.org/sites/default/files/B2S%202021%20-
%20Full%20Toolkit.pdf
Model School District Policy on Suicide Prevention hps://afsp.org/model-school-policy-on-
suicide-prevention
National School Mental Health Curriculum and Best Practices for States, Districts, and
Schools
hps://mhcnetwork.org/centers/mhc-network-coordinating-oice/national-
school-mental-health-projects
National Child Traumatic Stress Network’s Trauma-Informed School Strategies During Covid-
19 hps://www.nctsn.org/resources/trauma-informed-school-strategies-during-covid-19
NM Connect hps://nmcrisisline.com/nmconnect-app
Protecting Youth Mental Health, U.S. Surgeon General’s Advisory
hps://www.hhs.gov/sites/default/files/surgeon-general-youth-mental-health-advisory.pdf
Psychological First Aid for Schools (PFA-S) hps://rems.ed.gov/K12PFAS.aspx
Suicide Prevention Resource Center hps://www.sprc.org
The Sky Center’s Adolescent Hugs Program hps://skycenter.nmsip.org/our-
programs/adolescent-hugs
US Department of Health and Human Services, Stop Bullying Campaign
hps://www.stopbullying.gov

59
Appendix F: New Mexico Rule for Small Numbers and Public Data Release
New Mexico Rule for Small Numbers and Public Data Release
Specified population/
Event set*
Numerator
Action
<20 AND 1-3 Suppress (and suppress other
cells allowing calculation of 1-3)
>=20
all
Release
*Event set – the set of which the numerator is an immediate subset
Percentages or rates that can be used to determine the value of suppressed cells must also
be suppressed.
These guidelines do not relieve the data user of the responsibility to be aware of the
confidentiality issues regarding the data and to appropriately present data.
Do not suppress the number of births or deaths at the state, district, or county levels
presented by standard racial/ethnic groups, standard age groups, sex, prenatal care, birth
weight categories, birth order, plurality, total anomalies, marital status, or NCHS standard 113
cause of death categories.
Survey Data
If the number of persons surveyed in a given population or subpopulation is 50 or greater
then estimates based on this surveyed population or subpopulation will not be suppressed.
It is recommended that confidence intervals for the estimate be presented.

60
Appendix G: Related Resources
2022 Data Book | New Mexico Human Services Department
hps://www.hsd.state.nm.us/2022-data-book
Centers for Disease Control and Prevention hps://www.cdc.gov
Adverse Childhood Experiences (ACEs)
hps://www.cdc.gov/violenceprevention/aces/index.html
Child Abuse and Neglect Prevention
hps://www.cdc.gov/violenceprevention/childabuseandneglect/index.html
Firearm Violence Prevention
hps://www.cdc.gov/violenceprevention/firearms/index.html
National Center for Injury Prevention & Control hps://www.cdc.gov/injury
Sudden Unexpected Infant Death and Sudden Infant Death Syndrome
hps://www.cdc.gov/sids/index.htm
Suicide Prevention hps://www.cdc.gov/suicide
The Public Health Approach to Violence Prevention
hps://www.cdc.gov/violenceprevention/about/publichealthapproach.html
The Social-Ecological Model: A Framework for Prevention
hps://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html
Comprehensive Report on Gunshot Victims Presenting at Hospitals in New Mexico, 2023
hps://www.nmhealth.org/publication/view/report/8463
Connect New Mexico hps://connect.nm.gov
Kids Count (Annie E Casey Foundation) hps://www.aecf.org/resources/2022-kids-count-
data-book
National Center for Fatality Review and Prevention hps://ncfrp.org
New Mexico Indicator Based Information System (NM-IBIS) hps://ibis.doh.nm.gov
New Mexico Maternal Mortality Review Report, 2022
hps://www.nmhealth.org/data/view/maternal/2684
New Mexico Oice of the Medical Investigator hps://hsc.unm.edu/omi
New Mexico Oice of the Medical Investigator, 2021 Annual Report
hps://hsc.unm.edu/omi/_docs/pdfs/ar2021.pdf
New Mexico Pregnancy Risk Assessment and Monitoring System (NM PRAMS)
hps://www.nmhealth.org/about/phd/fhb/prams
New Mexico Voices for Children Kids Count Data Book hps://www.nmvoices.org/wp-
content/uploads/2022/01/KidsCount-DataBook2021-FINAL.pdf
New Mexico Youth Risk & Resiliency Survey hps://youthrisk.org
Safe Sleep NM hps://www.safesleepnm.org
Safe Storage NM hp://www.safestoragenm.org
State of Mental Health in New Mexico, 2022
hps://www.nmhealth.org/data/view/report/2650
Substance Use and Mental Health Services Administration hps://www.samhsa.gov
988 Suicide & Crisis Lifeline hps://www.samhsa.gov/find-help/988

62
References
Centers for Disease Control and Prevention. (2021, April 6).
About the CDC-Kaiser Ace Study
|Violence prevention injury Center CDC
. Adverse Childhood Experiences. Retrieved
December 17, 2022, from hps://www.cdc.gov/violenceprevention/aces/about.html
Centers for Disease Control and Prevention. (2022, November 2).
Disparities in suicide
. Facts
About Suicide. Retrieved December 26, 2022, from
hps://www.cdc.gov/suicide/facts/disparities-in-suicide.html
Centers for Disease Control and Prevention (2021, December 3).
Economic Cost of Injury —
United States, 2019
. Retrieved December 8, 2023, from
hps://www.cdc.gov/mmwr/volumes/70/wr/mm7048a1.htm?s_cid=mm7048a1_w
Centers for Disease Control and Prevention (2023, September 15).
Social Determinants of
Health
Retrieved November 28,2023, from
hps://www.cdc.gov/publichealthgateway/sdoh/index.html
Centers for Disease Control and Prevention (2023, June 29).
Adverse Childhood Experiences
(ACEs)
Retrieved December 1, 2023, from
hps://www.cdc.gov/violenceprevention/aces/index.html
Curry, S. R. (2017).
Childhood experiences and housing insecurity in adulthood: The salience
of childhood emotional abuse.
Children and youth services review, 82, 301-309.
Gardner, J. W., & Sanborn, J. S. (1990). Years of potential life lost (YPLL)—what does it
measure? Epidemiology, 322-329.
Jonson-Reid, M., Cheng, S.-Y., Shires, M. K., & Drake, B. (2022).
Child fatality in families with
prior CPS history: Do those with and without intimate partner violence dier?
Journal
of Family Violence. hps://doi.org/10.1007/s10896-022-00383-9
Moon, R. Y., Carlin, R. F., Hand, I., & Task Force on Sudden Infant Death Syndrome and the
Commiee on Fetus and Newborn. (2022).
Evidence base for 2022 updated
recommendations for a safe infant sleeping environment to reduce the risk of sleep-
related infant deaths.
Pediatrics, 150(1), e2022057991.
National Center for Fatality Review and Prevention. (2022, June).
National Fatality Review
Case Reporting System User Manual version 6.0.
Retrieved December 30, 2022, from
hps://data.ncfrp.org/Content/Files/UserManualVersion6.pdf
Kniesner, T. J., & Viscusi, W. K. (2019).
The value of a statistical life.
Forthcoming, Oxford
Research Encyclopedia of Economics and Finance, Vanderbilt Law Research Paper,
(19- 15).
Sokol, R., Austin, A., Chandler, C., Byrum, E., Bousquee, J., Lancaster, C., ... & Shanahan, M.
(2019).
Screening children for social determinants of health: a systematic review.
Pediatrics, 144(4).
Schneider, S. (2020).
Associations between childhood exposure to community violence,
child maltreatment and school outcomes.
Child abuse & neglect, 104, 104473.
U.S. Department of Health and Human Services, Oice of Disease Prevention and Health
Promotion.
Healthy People 2030,
Retrieved November 28,2023, from
hps://health.gov/healthypeople/objectives-and-data/social-determinants-health

64
NM-CFR 2023 Report Tear Sheet
The following two pages are intended to be used as a one-page summary resource. Whether
this document is printed in its entirety or pages 65 and 66 are printed alone, print on both
sides for optimal use.

PLACE OF INCIDENT
NM-CHILD FATALITY REVIEW
2023 ANNUAL REPORT
SELECTED FINDINGS
NM VS US TRENDS
The child injury death rate in New Mexico has consistently been higher than the national rate.
In 2021, the injury related child death rate in NM was 23 per 100,000 population, compared to 14.4
per 100,000 population in the US.
MANNER OF DEATH BY AGE
O F F I C E O F I N J U R Y & V I O L E N C E P R E V E N T I O N | N M D O H
RISK & PROTECTIVE FACTORS
Across its’ panels, the following risk and protective
factors were observed:
Access to Lethal Means
Adverse Childhood Experiences, Life Stressors
Child and Mental Health
Lack of Supervision, Child Maltreatment
Socioeconomic Status
13
PREVENTABILITY
If an individual or the community could
reasonably have done something that
would have changed the circumstances
that led to the child's death.
Of the 84 unique child deaths
reviewed in 2022, NM-CFR determined:
79.76%
could have been prevented
2.38%
could not be prevented
5.95%
unable to determine
MOST CHILD DEATHS IN NM ARE UNINTENTIONAL
More than 35% of all child deaths (0-17) were by Unintentional Injury.
From 2011-2021, 589 child fatalities in NM were unintentional injuries. These deaths are due to
motor vehicle crashes, drownings, unintentional overdose or poisonings, fire or environmentally
related, and other unintentional injuries.

Read the full report
NM-CHILD FATALITY REVIEW
2023 ANNUAL REPORT
SELECTED RECOMMENDATIONS
TO INCREASE BEHAVIORAL HEALTHCARE & ACCESS TO RESOURCES:
CYFD, ECECD, DOH & PED should require suicide prevention gatekeeper
training, such as QPR (Question. Persuade. Refer.) ™ or Mental Health First
Aid for appropriate personnel, as well as personnel in state-funded child-
serving organizations, including public schools, behavioral health care
settings, medical care settings & childcare settings.
The NM-CFR supports the implementation of a centralized reporting and
referral database that can be utilized by state agencies, police
departments, medical providers, and other partners to flag and assist
children who are being exposed to violence and need referrals, especially
mental health.
TO STRENGTHEN THE NM-CFR FOR IMPROVED DATA &RECOMMENDATIONS:
The NM Legislature should appropriate recurring funding to support the NM Child
Fatality Review in its programmatic operations and activities.
State agencies, NM-CFR Panelists, policymakers, the media, and the public should
disseminate this report and its findings widely, in remembrance of those it
describes, and to increase awareness of the burden of child fatality in New
Mexico, as well as prevention efforts.
TO INCREASE SAFE HOME ENVIRONMENTS:
The NM Legislature should pass legislation that requires hospitals, birthing facilities, midwives
& birth workers to provide education to parents/caregivers about safe infant sleep practices,
as prescribed by the American Academy of Pediatrics, & training for appropriate personnel in
state-funded infant-serving organizations, including childcare facilities & departments such as
ECECD and CYFD.
Child-serving agencies and organizations should implement policy and make available
resources to improve safe home environments for families, such as gun locks, baby gates and
products to encourage safe infant sleep practices, smoke and carbon monoxide detectors and
airway clearing devices.
O F F I C E O F I N J U R Y & V I O L E N C E P R E V E N T I O N | N M D O H
